
Quality by Design and Risk-Based Monitoring

Publication Date: February 2015 / Download PDF
Authors: Ibtissem Triki and Vanessa Towers
Brief Background
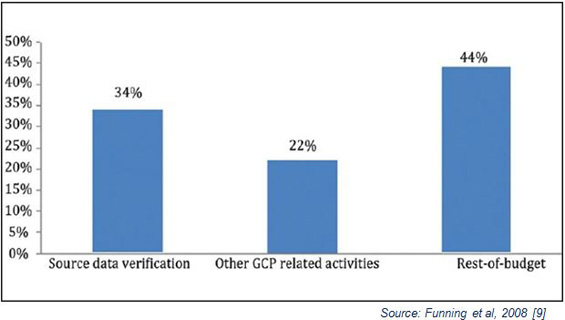
Over the past decade, the clinical research industry’s standard to meet regulatory monitoring obligations has involved frequent and regular onsite monitoring visits with 100% source data verification (SDV). The belief that “more is better” continues even with new evidence that on-site monitoring practices do not necessarily guarantee patient safety and data quality. An electronic survey was conducted by the Clinical Trials Transformation Initiative (CTTI) in 2008 to assess the clinical monitoring practices utilized across different types of organizations involved in clinical research. The results published in 2011 have highlighted the heterogeneity in monitoring practices between clinical trial organizations, and the key conclusion is that traditional monitoring is inefficient and doesn’t always lead to increased patient safety and data quality in clinical trials.
Current State
More recently, regulatory agencies have issued guidelines, documents and reflection papers to encourage our industry to adopt strategies that reflect a risk-based monitoring approach using a combination of monitoring strategies and activities. The following is a short list of these issuances:
- Medicines and Healthcare Products Regulatory Agency (MHRA)/Medical Research Council (MRC), and Department of Health (DH) in United Kingdom: Risk-adapted Approaches to the Management of Clinical Trials of Investigational Medicinal Products (2011) [1];
- Food and Drug Administration (FDA): Guidance for Risk-Based Approach to Monitoring (2013) [2];
- European Medicines Agency (EMA): Reflection paper on risk based quality management in clinical trials (2013) [3].
Based on the results of a new survey conducted by the Avoca Group [4][5], Risk-based Monitoring (RBM) has gained great interest within the industry, since 67% of the Sponsor companies have applied RBM to outsourced clinical trials (with variable frequency), while 33 % have never applied RBM (Figure 1). It also outlined that pharmaceutical and biotechnology companies are in various stages of implementing RBM programs, and that the impact of using RBM methodology on the efficiency and the quality of the clinical trials differs from one organization to another (Figure 2).

Risk-Based Monitoring Methodologies
Transcelerate Biopharma’s “Position Paper on Risk based Monitoring Methodology”, the FDA Guidance for Industry “A Risk-Based Approach to Monitoring” and the EMA Reflection Paper on “Risk Based Quality Management in Clinical Trials” have all proposed new models to encourage our industry to shift from inefficient and costly traditional monitoring practices to a risk-based monitoring approach using a combination of monitoring strategies and activities. This also highlights the fact that “one model does not fit all” when it comes to implementation of RBM methodologies. Ultimately, your organization has to determine the best combination of RBM methods for your operational needs and customer expectations. Moreover, these guidance highlight the importance of building quality into both scientific design and conduct of clinical trials by applying the Quality by Design concept (FDA) or the Risk based quality management processes (EMA).

Quality by Design and Quality Risk Management
“Quality by Design” (QbD) has been successfully applied in the Drug manufacturing process [6] for many decades. In the clinical trial development world, a QbD approach ensures that the planning, conduct, analysis and reporting of clinical trials are done in a way that eliminates significant errors. Quality Risk Management (QRM) identifies risks and takes steps to control the risks and review these results to improve quality.
Key Risk Indicator (KRIs)
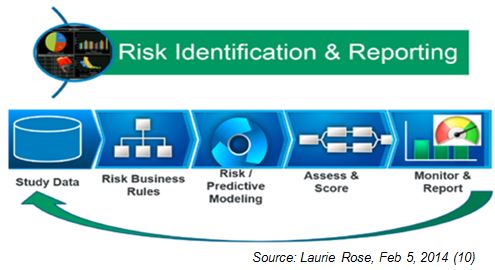
Recently, TransCelerate BioPharma had developed a Risk Assessment Categorization Tool (RACT) to manage clinical trial risks through identification, categorization (High, medium, or low) and appropriate mitigation [7]. Each study is categorized with an overall risk level that will vary during the study progress. As part of an RBM methodology, KRIs allow for the documentation of issues and risks, as well as the corrective actions and preventive plans in response to those risks.
![]()
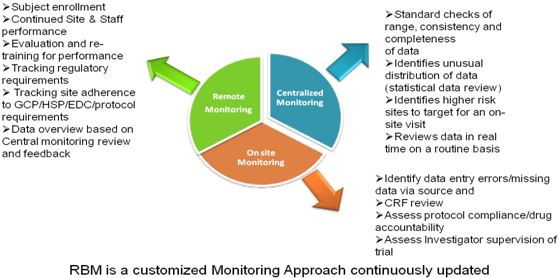
RBM is not a matter of reducing the amount of monitoring, but is more focused on using more efficient methods to improve effectiveness using a combination of different types of monitoring approaches such as:
- Centralized or remote monitoring;
- On-site monitoring visits.
The Importance of RBM Plans
RBM is part of an integrated approach of quality by design and risk assessment approaches throughout the entire project lifecycle. As stated in the FDA guidance, risk based monitoring plans should be customized for every clinical trial to ensure that cross-functional teams focus on the risks that are most important to subject safety, data quality and regulatory compliance.
RBM Benefits
Implementing RBM approaches allows for significant time and project cost savings along with increasing quality metrics.
There is growing empirical evidence that reduced or targeted appropriation of resources may produce the same or a higher level of study data quality compared with extensive monitoring incorporating full source data verification. Overview of study data in real time through a centralized process helps to proactively manage clinical trials. Any issues or problems with study data can be detected immediately and corrected quickly in order to protect patient safety and data integrity.
Implementing Risk-based methodology allows monitors to focus more on site management, data trends, and patients with higher risks of errors or non-compliance. This in turn improves the CRA’s productivity by concentrating on high risk issues rather than low risk ones.
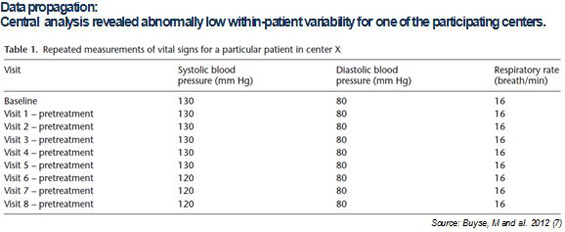
Central monitoring can reveal issues with data such as data propagation, biased scores, or even instances of fraud that were not detected during on-site visits [8].
Cost Benefit: RBM allows sponsors to send fewer CRAs to low-risk sites and focus more on high risk sites. This typically reduces the number of CRAs needed to monitor an entire trial and also decreases the cost of associated travel expenses.
Saving Time: Reducing the amount of SDV can save time overall. Additionally, conducting targeted monitoring of sites which have higher risks in order to prevent low data quality, in turn, decreases the amount of data cleaning to be performed as well as the time required for database closure.
RBM does not suggest that monitors should only conduct site visits when there is a problem. On site monitoring visits are still needed to help build and maintain a good working relationship between the monitor and the site team. Virtual oversight may hinder the monitor’s ability to develop the instinct to detect less obvious but more significant issues at a site. Remote metrics may not be sufficient to detect abnormal trends or patterns in the data and this gives the monitor a false sense of security. Therefore, they may miss some types of fraud or serious errors that can be detected during site visits – made evident in hand-written documents, or by interviews with site personnel.
Vantage BioTrials has the core competency for risk-based monitoring that helps Sponsors manage clinical trials with a high degree of efficiency. We offer a comprehensive and compliant solution to proactively assess risks throughout the trial’s lifecycle and implement logic based workflows to identify issues, reduce risks and improve overall quality and compliance. Our risk based monitoring process helps mitigate risks associated with studies that could jeopardize data integrity.
References
- MRC/DH/MHRA Joint Project. Risk-adapted Approaches to the Management of Clinical Trials of Investigational Medicinal Products, 2011.
- Food and Drug Administration. Guidance for Industry Oversight of Clinical Investigations -A Risk-Based Approach to Monitoring, 2013.
- European Medicines Agency: Reflection paper on risk based quality management in clinical trials, 2013
- The Avoca Group, The State of Clinical Outsourcing: Managed Risk in Outsourced Clinical Trials, DIA Annual Meeting, June 24, 2013.
- Wang and al. Shifting Monitoring Paradigms: Challenges and Opportunities. Applied Clinical Trials: Jun 1, 2014.
- John Avellanet. Why Quality by Design? Cerulean Associates LLC, 2008.
- Position Paper: Risk-Based Monitoring Methodology. TransCelerate BioPharma Inc., 30 May 2013.
- Buyse, and al. A statistical approach to central monitoring of data quality in clinical trials. Applied Clinical Trials : 8 June 2012
- Funning et al., Quality Assurance Journal, 2008.
- Laurie Rose. Risk-Based Monitoring Key to Protecting Data Integrity and Improving Patient Safety Publish Date: Feb 5, 2014